Blood proteins and their use in equine biochemistry profiles
by Dr. Stacey A. Newton, Lead Clinical Pathologist, NationWide Laboratories
Case study: Large granular lymphocyte lymphoma
by Dante Meza Ruiz Associate Pathologist, NationWide Laboratories
Pathology Focus
This lecture, presented by Dr. Stacey A. Newton, Lead Clinical Pathologist at NationWide Laboratories, explores the critical role of blood proteins in equine biochemistry profiles, emphasising their diagnostic and monitoring applications. It highlights proteins' biological functions and their use in evaluating health and disease in horses.
Key topics include acute phase proteins (APPs), their response to inflammation, and the interpretation of albumin and globulin levels in clinical contexts. Special attention is given to the diagnostic utility of APPs like serum amyloid A and fibrinogen in detecting and monitoring inflammatory and neoplastic conditions. The lecture also delves into advanced diagnostic techniques like serum protein electrophoresis to assess protein fractions and identify disease processes. Practical insights into the clinical significance of hyperproteinemia, hypoalbuminemia, and hyperglobulinemia enrich this comprehensive presentation, making it indispensable for equine veterinary practitioners.
Integrate into practice: Incorporate protein analysis into routine diagnostics to enhance the management of equine health and disease
Apply advanced techniques: Employ serum protein electrophoresis for detailed examination of globulin fractions and disease diagnostics
Diagnose using APPs: Utilise acute phase proteins such as serum amyloid A and fibrinogen to identify and monitor inflammation and tissue damage
Interpret biochemistry profiles: Analyse albumin, globulin, and APP levels to diagnose inflammation, neoplasia, and other disorders
Understand blood proteins: Recognise the fundamental functions of blood proteins and their role in equine physiology and pathology
Watch now
Pathology Case Study
By Dante Meza Ruiz Associate Pathologistat NationWide Laboratories,DVM, M.Ed., DVSc, Dipl. ACVP/ASVCP
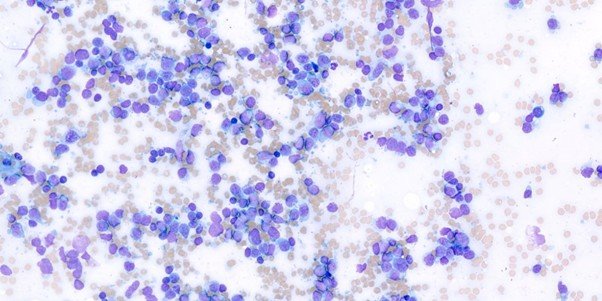
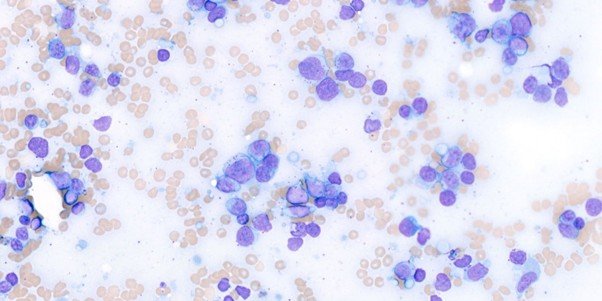
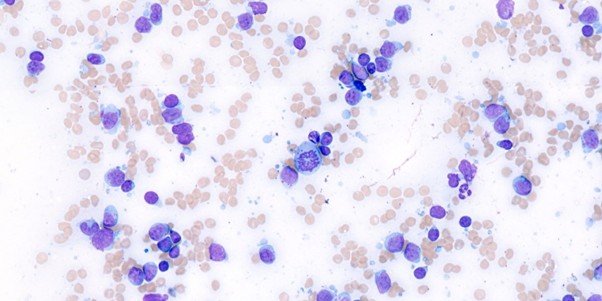
A 12-year-old spayed female Beagle was presented to a veterinary clinic with a history of a golf ball-sized mass on the neck. A fine-needle aspiration (FNA) was performed, and the sample was submitted to NationWide Laboratories for evaluation.
The sample was highly cellular and mildly hemorrhagic. It was predominantly composed of a monomorphic population of intermediate to large lymphocytes. These cells displayed scant to moderate amounts of pale blue cytoplasm, often containing multiple magenta granules. The nuclei were round to angular, occasionally cleaved, with finely stippled chromatin and one to two nucleoli observed in some cells. Occasional mitotic figures were present. Scattered throughout the sample were a few small lymphocytes and rare plasma cells.
A diagnosis of lymphoma was established, and based on the cytological characteristics of the cells, it was classified as a large granular lymphocyte lymphoma (LGLL).
Canine lymphoma is a heterogeneous disease with variable clinical presentations, morphologic features, and biological behaviour. Subtyping lymphoma according to the World Health Organisation (WHO) classification can assist in guiding treatment decisions and predicting prognosis1.
Large granular lymphocytes (LGLs) are a type of intermediate to large, lymphocyte distinguished by their prominent azurophilic cytoplasmic granules. They originate from either cytotoxic T cells (T-LGL) or natural killer (NK) cells (NK-LGL). In dogs, granular lymphocyte neoplasia most frequently manifests as chronic lymphocytic leukaemia (CLL)2.
Canine large granular lymphocyte lymphoma (LGLL) is rarely reported, with extra-nodal presentations and a T-cell immunophenotype being most common. Among these, hepatosplenic involvement is the most frequently observed form, frequently originating from CD11d+ TCRγδ-restricted LGLs within the splenic red pulp3. γδ T lymphocytes are primarily found in the spleen, though small numbers have also been identified in lymph nodes and certain epithelial-rich tissues. While their exact function remains unclear, they are thought to play a role in the first line of defence within the epidermal and mucosal epithelial barriers4.
Other reported primary sites for canine LGLL include peripheral lymph nodes, skeletal muscle, mediastinum, skin, urinary bladder, small intestine, and kidney. Due to the variability in clinical presentations and treatment protocols described in the current literature, an optimal treatment approach for canine LGLL has yet to be established 3. Nevertheless, canine LGLL appears to follow an aggressive clinical course, with most dogs presenting at diagnosis with substage b disease (exhibiting clinical signs of illness).
While hypercalcemia is a common contributor to clinical signs in dogs with T-cell lymphoma, a recent study on LGLL found that only a small proportion of affected dogs were hypercalcaemic. This suggests that hypercalcemia is unlikely to be a major factor in the high frequency of clinical signs observed in these cases 3.
Haematological abnormalities are commonly observed in cases of LGLL, with anaemia, neutrophilia/neutropenia, monocytosis, and thrombocytopenia frequently reported. Although the underlying mechanisms are not fully understood, potential contributing factors include bone marrow involvement, haemophagocytic syndrome, immune dysregulation, and elevated inflammatory biomarkers, all of which have been previously associated with a poorer prognosis5.
Unfortunately, no additional clinical history or further diagnostic testing was provided to the laboratory, and information regarding the outcome of the case is unavailable. However, based on previously reported cases, this form of lymphoma is considered aggressive and is typically associated with a short median progression-free interval and overall survival time. Currently, the optimal management approach for canine LGLL has not been determined.
Click here for references
Read more case studies from NationWide Laboratories